Landing Biomechanics, Injury Risk & Dynamic Taping
How might knee injury risk be reduced with Dynamic Taping?
In the previous newsletter, the award winning study by Robinson et al which investigated the impact of Dynamic Taping to the hip on a Greater Trochanteric Pain Syndrome (GTPS) group was reviewed. This study showed that Dynamic Taping, when applied in a shortened position to resist hip flexion/adduction/internal rotation had the greatest impact on velocity and magnitude of hip frontal and transverse plane motion and pelvic obliquity during walking gait, and resulted in a significant reduction in pain.
This month, we consider the impact that similar techniques have on the knee and briefly consider other factors that may also be contributing to injury risk based on the movement profile.
A recent study by Chih-Kuan Wu and colleagues (2022) (https://doi.org/10.3390/ijerph192013716) investigated the influence of hip extension, external rotation and abduction taping on landing biomechanics in young volleyballers using a jump-landing task. Landing Error Scoring System (LESS) and Anterior-Posterior Knee Laxity under 20lbs and 30lbs loads were evaluated. 42 high schools students (21 male and 21 female) who were free from knee injury and had no history of ACL injury or reconstruction, all participating in volleyball five days per week were included in the study.
Results showed that in addition to improving knee laxity, Dynamic Taping significantly reduced landing errors in both sexes, females more than males. Similarly, those with higher risk scores pre-tape had a larger benefit. Scores were essentially aligned with the minimally clinically important difference score identified in previous studies.
How could the risk be reduced further across the population based on observations in this study?
- Examination of the photo of the technique (Figure 1) shows that the tape passes superior to the hip joint posteriorly thereby exerting minimum extension force. This also means that the tape does not tighten as much during hip flexion on landing and thereby does not resist motion in the other planes as much as it could. Slight changes to the technique would increase it’s effect.
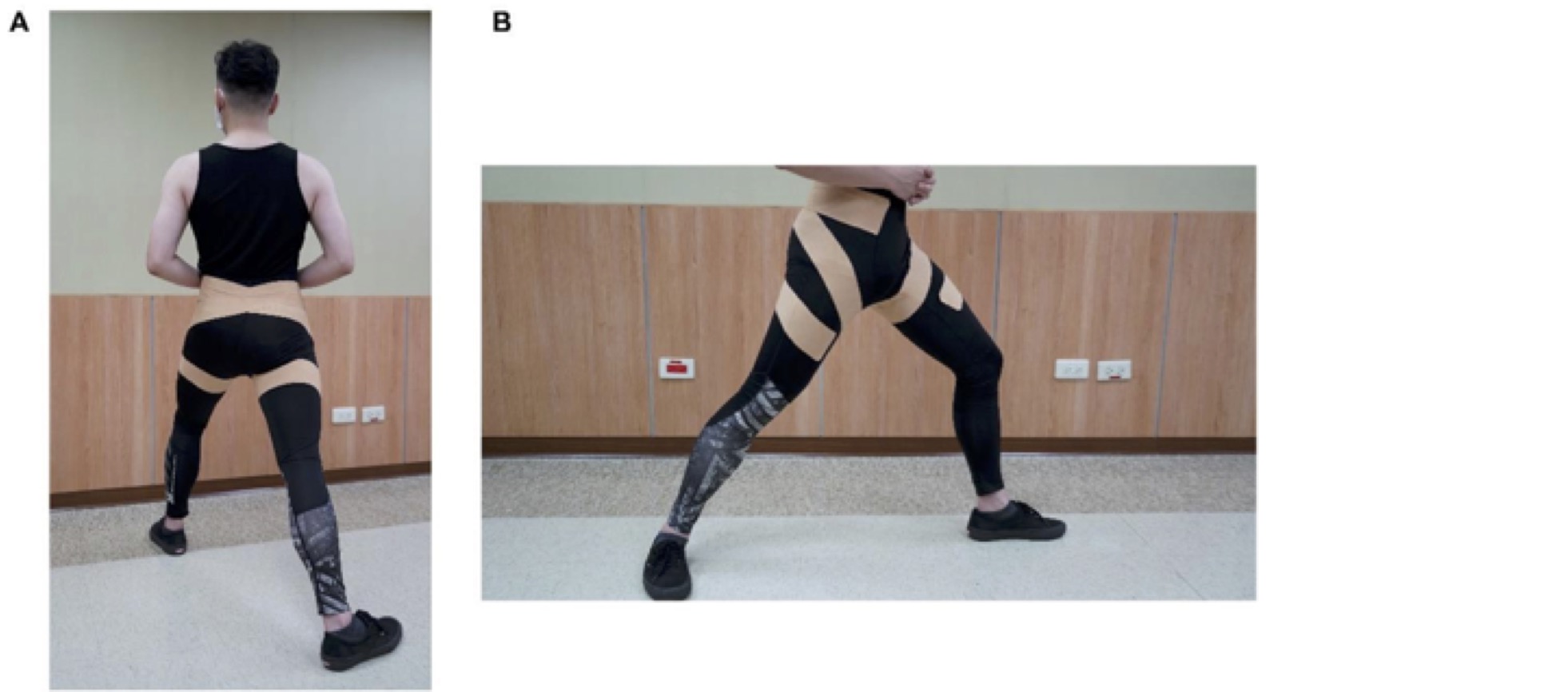
Figure 1. The photos from the study show and describe the technique crossing the lower back. Crossing the hip joint posteriorly i.e. bringing the oblique section distally will result in greater hip extension moment and tighten the tape during hip flexion to also generate more resistance to adduction and internal rotation
- The reason for the increased risk movement has not been identified. The hip has been the target for taping in each subject however it may be poor quads action and sagittal plane knee control that is resulting in the compensatory hip adduction and internal rotation. In such a case, creating a knee extension force to help address the deficit is likely to yield better changes at both the hip and knee. Similarly, changes at the foot may impact Dynamic Valgus at the knee with preliminary research showing that Dynamic Taping for arch support can address this.
- Identifying those with movement suggestive of greater risk rather than just taping everyone results in bigger changes i.e. tape those who need it, where they need it.
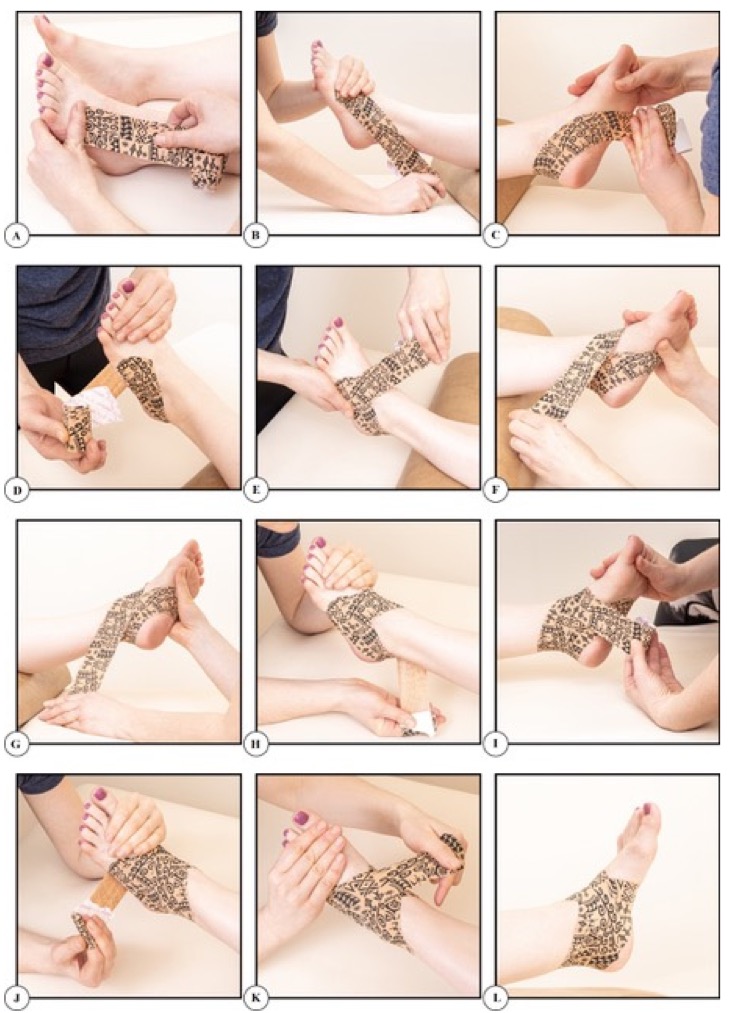
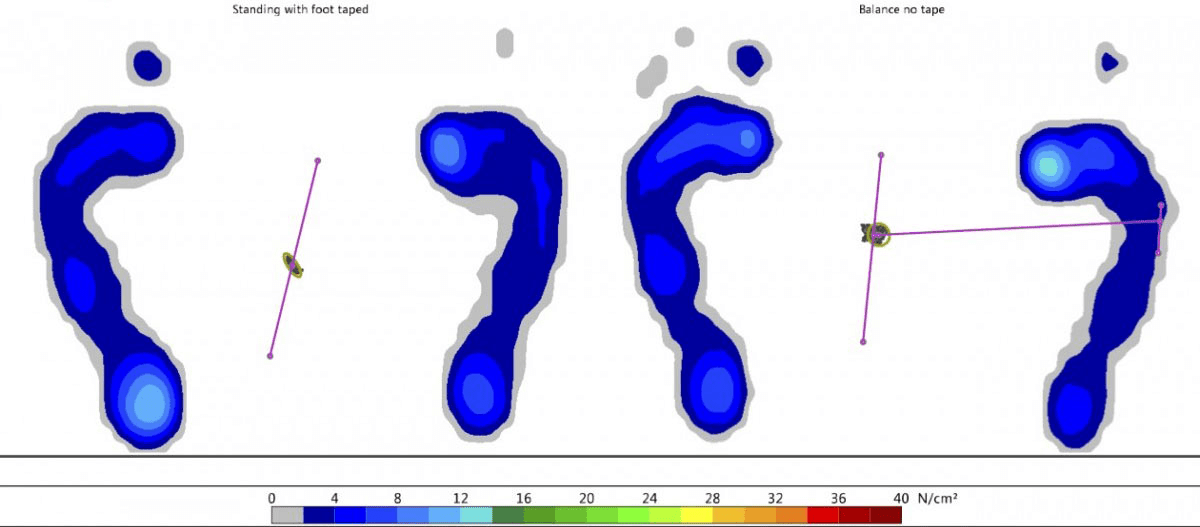
A study by Mehmet Donmez (supplied) showed that Dynamic Taping for arch support in volleyballers with a low medial longitudinal arch reduced dynamic valgus at the knee in a Single Leg Squat Test, Vertical Jump Drop Test and Single Leg Drop Test when compared to sham tape (Dynamic Tape Global applied in a lengthened position) and no tape. Further support highlighting the various contributors is provided by Eva Ilie et al(https://ibn.idsi.md/vizualizare_articol/119875) who showed that Dynamic Taping for knee extension resulted in increased Single Leg Squat Test in a group of 13 subjects with various knee injuries and pain including ACL injury and ACL reconstruction.
Bittencourt et al, 2016 (https://bjsm.bmj.com/content/51/4/297.3) in BJSM provide further support showing that the hip technique resulted in significant changes to high frontal plane knee projection angles (FPKPA) in elite female volleyballers during a single leg squat task. Pre-tape mean FPKPA of 10.5º was reduced to 5.4º bringing it below the risk threshold.
Once again it is worth remembering that it is always n=1 when assessing and managing your patient or athlete. Thorough assessment and sound clinical reasoning is required to identify clear indications and appropriate application of the research. Correct application of the technique (short position, correct line of pull relative to the axis, tension) are required to get maximum mechanical effect and improvement in the parameters measured associated with a reduction in injury risk.